Hello to everyone and thank you for
your generous support. These are very difficult times for medical
research, especially for rare conditions like
achondroplasia/hypochondroplasia. The National Institutes of Health,
which funds most medical research in the U.S., has had its budget cut even
further with the sequester. Less than 10% of grants are funded now and
droves of people are leaving research. Please tell your congressmen and
senators to restore funding to the NIH!
On to research progress. The major
thing occupying our time right now is the drug screen.
How do we do it?
Let me explain how cartilage behaves
first. You find cartilage in your ears and nose (elastic cartilage
because it bends), your joints (look at a chicken leg bone- the white, shiny
part is the joint cartilage), and in the growing parts of the bone in
children. The way children grow in height is by making cartilage grow and
turning it into bone (we call it the growth plate). For example, in your thigh
bone children have two growth plates- the one near your hip and the one near
your knee. See the figure below:
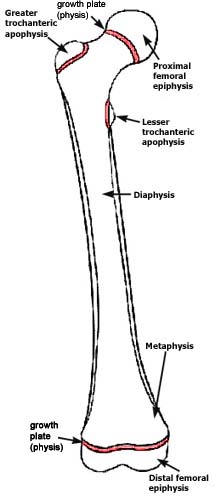
Thigh
bone (femur) of a growing child. The hip is at the top where the ball
is and the knee at the bottom. The growth plates are marked and
colored.
|
Growth plates look simple
under the microscope but are very complicated organs. Cartilage cells
(the pink/blue dots in the figure below) are surrounded by the proteins that
they make. The protein consists of collagens that hold the cartilage
together and make it tough and other proteins (proteoglycans) that have a lot
of complex chains of sugar attached to them. Proteoglycans attract water
and so these proteins make cartilage cushion better (like when you put pressure
on your joints while walking and running). Farthest away from the bone
are the resting cartilage cells that are less active and are the reserve (like
players waiting on the bench). The resting cells receive signals to
divide and columns of dividing cells are formed in the proliferating
zone. They then receive additional signals and stop dividing and enlarge
in size significantly in the hypertrophic zone closest to where new bone is
formed. These large cartilage cells produce calcium crystals around
them. Finally, these large cartilage cells die and protein containing
calcium that they have made is replaced by regular bone. This whole
process is called endochondral ossification.
In achondroplasia and
hypochondroplasia, the cartilage cells don't divide as fast, there is less
protein between the cells, and the cells don't turn into hypertrophic zone
cells very well. All this causes the growth plate to be shortened and
growth in children to be slowed.

Growth
plates of a normal child (control on the left) and of a severe cousin of
achondroplasia (thanatophoric dysplasia, on the right). The newly
formed bone would be at the bottom.
|
Fibroblast growth factor receptor 3 (FGFR3) acts as a brake for cartilage cells in the growth plate. The genetic mutations that cause achondroplasia and hypochondroplasia increase the strength of the brake. The way that the drug being tested by BioMarin works is to partially release the brake. It can't release it all the way because it is only able to counteract part of what FGFR3 does. That is why we are trying to find another medication using a drug screen.
For years, we have been using RCS
cartilage cells to study how FGFR3 works. RCS cells are cartilage cells
that grow very well in a culture dish. They have a lot of FGFR3. In
a culture dish, they normally look like round balls surrounded by a soft layer
of cartilage proteins.
In the figure below, the control
pictures are RCS cells grown in the culture dish. On the bottom is what
they look like with regular light. On the top we have stained them with
alcian blue, which is a stain for proteoglycans. When we add fibroblast
growth factor (FGF2), we turn on FGFR3. With FGF2 you can see the cells
have flattened out, attaching to the plastic at the bottom of the culture dish
and no longer stain bright blue. The cells have stopped growing,
destroyed the proteoglycans around them, and changed their behavior. They
are more like primitive cells that haven't become cartilage cells yet.
Similar things are happening in the cartilage of children with
achondroplasia. If you treat the cells with a drug that blocks some of
what FGFR3 does, you get improved growth. You can see that CNP (related
to BioMarin's drug) helps the cells act more normally.

You can use the RCS system to find
new drugs. Add a drug to RCS cells and treat them with FGF2. If
they grow better, you have a promising compound to test further. The
really nice part about using this way to find drugs is if the drug is toxic to
cartilage cells, they cells won't grow better. Eliminating toxic drugs is
the usual headache for any drug screen.
To test our system, we used this RCS
system to screen 5000 compounds. We did it by hand in a square plastic
plate with 96 holes in it. Cells are put in each hole with different
drugs, FGF2 is added, and 3 days later we count cells. If there are more
cells, the drug may be doing something. We found one good compound from
this pilot screen, NF449. It works very well to block FGFR3 and isn't
toxic to the cells, but it would need modified to work well in humans. A
collaborator is trying to find where NF449 binds to FGFR3 so we can make those
modifications. Since developing any compound into a drug we can use in
people is a long-shot, we want to do a bigger drug screen of 100,000+
compounds.
Screening 100,000+ compounds by hand
would be very expensive and time consuming, so we are working with the drug screening
core facility at UCLA to use their robots.
In order to do the drug screen for
less than a fortune, we have to do it in plastic plates with 384 holes.
These holes are very tiny as you can see below compared to my index
finger. The cells grow at the bottom of the holes.

Unfortunately, we can't just take
the number of cells and the amount of FGF2 we used for the 96 well screen and
scale down to a smaller size. We have to test how many cells to use in
each well (too many and they don't want to divide, too few and you don't have
enough to measure) and how much FGF2 to use (too much and no drug could reverse
the growth arrest, too little and you don't get any growth arrest). We
had to work out how to measure the number of cells quickly and by robot (you
add a chemical that reacts with energy in cells and coverts it to light- the
more living cells, the more light). We had to make sure that the
conditions would still detect NF449 as a potential drug. We accomplished
all of that and then went to use the robots to do the grunt work. Darn it
if the tubing used to suck up the FGF2 solution from a bottle didn't bind all
the FGF2. No FGF2 in the tiny wells, the cells grow normally. This
kind of problem isn't unheard of, but it is annoying. We are working with
the screening lab director to solve this problem. Once it is solved and
we verify everything works well, then we are off to the races and can screen
all those drugs. Stay tuned!
Bill Wilcox